Rosacea is a skin condition often seen in conjunction with seborrheic dermatitis.
The condition seems to be genetic [1] and family history has been indicated in a large variety of cases [2], yet environmental factors appear to be equally important. Statistically, the condition seems to affect women more than men, but it appears more aggressive in men [3].
Similar to seborrheic dermatitis, rosacea has a tendency to spread and progress. Though the two conditions share many of their most prominent symptoms, they have major differences in their underlying causes and corresponding treatment approaches.
Most medical professionals will aim to achieve initial clearance followed by continuous management if issues persist; as opposed to achieving complete eradication.
Primary Symptoms of Rosacea
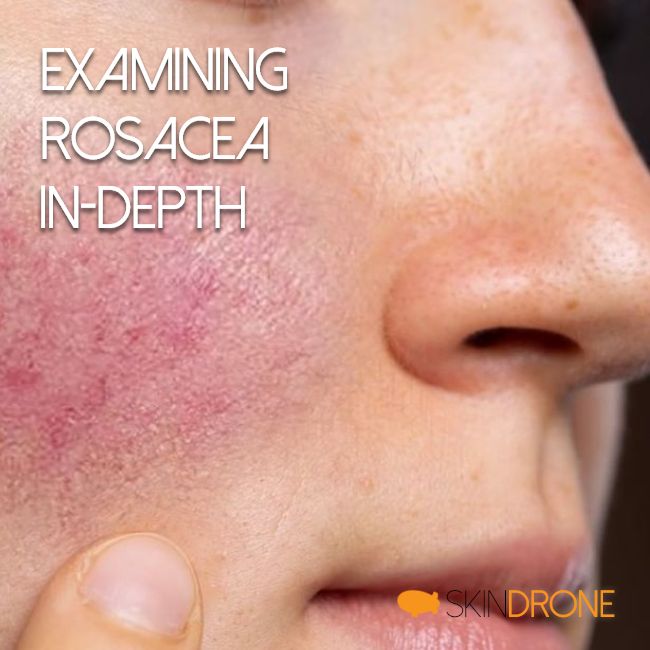
The most common symptoms seen in rosacea, include [4, 5]:
- Facial redness (erythema) in similar areas to that of seborrheic dermatitis
- Swollen red bumps on the skin (similar to acne)
- Eye issues (dryness, irritation, and itching)
- Flashes of heat (tingling and heat sensations of the skin)
- Visible blood vessels (also known as telangiectasia)
- Red nose
- Swelling (edema)
- Skin dryness (as a side-effect from overlapping skin issues)
The main difference here is that skin flaking and sebum production abnormalities are not primary symptoms of rosacea, as they are with seborrheic dermatitis.
Ruling Out Side-Effects of Topical Steroids
Individuals who apply topical steroids for extended periods of time can often demonstrate many of the primary symptoms present in rosacea [6, 7]. In these cases, the symptoms are considered to be side-effects and often reside on their own after a period of abstinence.
Similarity to Seborrheic Dermatitis
Though the underlying cause of rosacea symptoms and its progression differ from seborrheic dermatitis, the two conditions share some striking similarities.
Affected Area
Both conditions primarily affect the facial skin; resulting in a diminished sense of self-confidence and potential issues throughout social interactions. Many individuals often report this can lead to problems in employment, marriage and general interaction with other people.
Psychological Impact
Rosacea and seborrheic dermatitis are both known to have an immense psychological impact on the affected individual. In certain cases, this can lead to general depression and social withdrawal.
The Cyclical Nature of Stress
Due to the sensitive connection between stress and immune function, many researchers have speculated that the psychological aspect may be an integral part of the condition and contribute to its cyclical nature (stress -> skin issues -> stress)
Rosacea Basics
Similar to seborrheic dermatitis, rosacea is not yet fully understood by the medical community. Though the worldwide literature on the subject is abundant and growing every year, much confusion and uncertainty remain.
Unfortunately, much of this literature focuses on treatment approaches driven by companies funding the work and significant biases are evident [8]. The end result is that even though numerous modern treatment approaches have been proposed, a lack of fundamental understanding remains.
Rosacea Diagnosis
At this time, there are no official/standardized laboratory tests that can confirm or reject the presence of rosacea [8]. Primary diagnosis relies on the medical professionals understanding of common symptoms/sub-types and their ability to differentiate these symptoms from other overlapping conditions.
One thing that does appear to be of significant importance is not only identifying whether or not your symptoms represent rosacea, but also which sub-type of rosacea. Determining the specific sub-type will then allow for a more accurate selection of treatment approaches [9].
For example, individuals restricted to facial flushing, skin sensitivity, and redness; often report increased sensitivity to many topical treatment solutions. On the other hand, individuals that have accompanying skin bumps/pimples (pustules/papules), increased sebaceous production, and buttery fly pattern redness; are better able to tolerate topical treatment approaches.
Four Common Sub-Types
Though it was originally proposed that there are two main variants of rosacea (primarily characterized by either redness and flushing or papules and pustules), 4 subtypes have now been established.
- Erythematotelangiectatic rosacea
Skin flushing, persistent redness of certain areas and may include pronounced blood vessels. - Papulopustular rosacea
Same symptoms as primary sub-type above, but also featuring small bumps and papules. - Phymatous rosacea
Increased skin thickness and swelling; particularly of the nose, chin, forehead, cheeks, and ears. - Ocular rosacea
Ongoing eye irritation; including symptoms of burning, stinging, dryness itchiness, increased sensitivity to light, and pronounced redness.
Possible Causes of Rosacea
As mentioned throughout this section, the cause of rosacea symptoms remains elusive and no consensus has been reached. Nonetheless, there are certain factors of the condition which majority recent literature does appear to agree on.
Evidence suggests the following factors may play predominant roles:
- Vascular Abnormalities
Blood flow irregularities (most evident in the facial region, due to proximity to the skin surface) are evident [10] and may be related to abnormal hormone levels/production (vasoactive intestinal peptide [11], gastrin [12, 13], serotonin and/or histamine [14]). - Altered Innate Immunity
Antimicrobial peptides are used by the skin to defend against infection and injury [15]. They are used for cellular communication and play a key role in the inflammatory process. Abnormally high concentrations of the cathelicidins (an antimicrobial peptide) are seen in rosacea-affected skin and suggest an abnormal innate immune response [16, 17, 18]. - Climactic Exposures
Prolonged exposure of the skin to damaging environmental factors (such as high heat or UV radiation) may lead to chronic damage of cutaneous blood vessels and dermal connective tissue [10, 19, 20]. - Dermal Matrix Degeneration
Abnormalities in the inner lining of blood vessels [20, 21] and/or malfunctioning/damaged connective tissues [22, 23] are believed to result in structural changes of the skin, increased permeability of vessels and local pooling of blood, inflammatory mediators and metabolic waste products. - Ingested Chemicals and Foods
Spicy foods, alcohol, and hot beverages and known to trigger (not cause) rosacea flushes [24, 25], while certain medications (such as topical/nasal steroids, nicotinic acid, and high doses of vitamin B6) can either induce flashes or even produce rosacea-like symptoms [7, 26, 27, 28, 29, 30]. - Pilosebaceous Unit Abnormalities
Structural abnormalities of the pilosebaceous unit [23, 31] (consisting of the hair, hair follicle, arrector pili muscles and sebaceous gland) may lead to increased infiltration by inflammatory cells (such as neutrophils, eosinophils, lymphocytes, plasmacytes, macrophages and mast cells) and external antigens (Propionibacterium acnes and Demodex). - Demodex Mite Infestation
Demodex mite (present even on healthy skin) infestation of the hair follicle may play a critical role in rosacea progression [32, 33], but uncertainty remains [23, 31] and clinical improvement has been seen without reduction in demodex mite populations [34, 35]. - Helicobacter Pylori Infection
Possible connection between rosacea and gastrointestinal disease [36] has created suspicion that Helicobacter pylori infection may be the cause of rosacea in some individuals [37, 38, 39]. Studies evaluating the effectiveness of Helicobacter pylori eradication have shown mixed results [40, 41, 42] and some have hypothesized the overall effect of the antibiotic treatment may be responsible (not specifically the elimination of Helicobacter pylori) [43, 44].
Overall, there remain many uncertainties regarding the cause of rosacea. This is may be due to unknown factors not yet considered or the individuals differences amongst sufferers. Perhaps new technologies and findings in the future may make things more evident.
Rosacea Treatment Approaches
Due to rosacea’s complexity, no single treatment approach is guaranteed to produce complete clearance of symptoms. The majority of the literature on the subject suggests that rosacea is an incurable condition and ongoing management is required. Whether or not this is true, remains a subject of controversy and it’s possible that as new information comes to light, this opinion may change.
No matter what your opinion may be, reviewing the most common treatment approaches may still offer significant insight into the condition and some possibilities for near-term relief.
Some of the more common treatments include:
- Isolation and avoidance of triggering factors (diet, environment, medication, etc.)
- System antibiotics (tetracycline or metronidazole)
- Isotretinoin (Accutane)
- Topical antibiotics (metronidazole, clindamycin phosphate, permethrin)
- Topical retinoids and retinoid precursors (tretinoin or retinaldehyde)
- Sulfur (with or without sodium sulfacetamide)
- Azelaic acid
Many of which, are effective only at a portion of rosacea symptoms (such as facial redness or the pustules/papules) and treatments are often combined.
Avoiding Triggers
In the beginning stages of rosacea, many individuals report that isolating and reducing triggering factors may be the easiest approach to reducing overall symptom severity; with most potential in the area of reducing skin redness [45, 46].
Literature review suggests the following are some of the more common triggers [46]:
- Foods
- Liver and smoked meats
- Yogurt, sour cream and cheeses (excluding cottage cheese)
- Avocados, bananas, red plums, raisins, figs and citrus
- Eggplant, tomatoes, spinach, beans (lima and navy), peas
- Chocolate and vanilla
- Soy sauce and vinegar
- Hot and spicy foods
- Foods with high yeast content
- Beverages
- Alcohol (particularly red wine)
- Hot beverages
- Stress and anxiety
- Environmental
- Sun exposure
- Strong winds
- Excessively high or low humidity
- Excessively hot or cold temperature
- Skincare
- Formulations containing alcohol, witch hazel, fragrances, menthol, eucalyptus oil, clove oil, peppermint or sodium lauryl sulfate
- Harsh cleansers (such as regular soap)
- Over washing of the skin
- Aggressive exfoliation
- Medications
- Vasodilators
- Topical steroids
- Medical conditions
- Menopause
- Caffeine withdrawal syndrome
- Chronic cough
- Excessive physical exertion
Due to the long list above, trial and error are likely warranted to determine which specific factors are most influential in individuals cases. Interestingly, many seborrheic dermatitis sufferers report many of the same triggering factors.
One thing to keep in mind is that it may be necessary to be pragmatic (level headed) and not jump to conclusions when trying to isolate your triggers. Jumping from treatment to treatment may create unnecessary stress (which itself is one of the more common triggers) and get in the way of progress.
Systemic Antibiotics
Metronidazole and tetracycline have a long history in the treatment of rosacea [47, 48]. And at the time of this writing, doxycycline is the only FDA approved of the tetracyclines for the treatment of rosacea [49, 50].
Long term treatment is limited due to possible complications that can arise with ongoing antibiotic usage [51, 52, 53, 54] (particularly evident in tetracyclines usage) and potential for relapse upon ending treatment [55].
The main effects of oral antibiotics are seen on the pustules/papules of rosacea, with limited effects on the redness (erythema) component. If taking this route, careful consideration must be taken to determine the risk-benefit of such an approach and this is best done together with a qualified medical professional.
Antibacterial or Anti-inflammatory
It appears that the anti-inflammatory effects of antibiotics may be more closely related to symptom reduction then their antibacterial potential [56, 50].
Isotretinoin
Isotretinoin (a synthetic retinoid derived from retinol) is commonly used for the treatment of acne, but its effectiveness in rosacea treatment is evident [57, 58]. Though the clearest impact is seen on the papules and pustules [59], it also produces a noticeable reduction in redness [60, 61].
The issue with this treatment approach is that drug intolerance is fairly common and a variety of side-effects exists. Some of the most common side effects being mucosal dryness, inflammation of the lips (cheilitis), general skin inflammation (dermatitis), musculoskeletal pain, headaches and increased triglyceride levels (to name a few) [62, 63].
Topical Antibiotics
Topical antibiotics can help reduce the potential of side-effects seen in oral antibiotics by limiting the area of application and limiting exposure to only the affected areas. Nonetheless, the potential for developing antibiotic resistance remains present [64, 65].
Again, metronidazole and tetracycline appear to be two of the most popular options [66, 67] and come in several forms (creams, lotions, and gels). Other options include clindamycin phosphate and permethrin.
Topical Retinoids and Retinoid Precursors
In-line with the effectiveness seen with isotretinoin usage, attempts have been made to evaluate the effectiveness of topical approaches aimed at modulating retinol function.
Tretinoin is another retinoic acid commonly used for the treatment of acne and has shown potential for rosacea treatment. In the case of rosacea, topical usage compared favorably to systematic isotretinoin usage in reducing both papules/pustules and redness [68]. However, safety concerns still exist and adverse reactions are very common [69, 70]
Retinaldehyde, on the other hand, is a natural precursor and the skin/body needs to first convert it to either retinoic acid or retinal [71]. Studies appear to indicate it may be a safer and much better-tolerated alternative to tretinoin [72], while also producing a significant improvement of the skin redness component of rosacea [73].
Sulfur
Sulphur is arguably one of the more natural topical approaches for the treatment of rosacea discussed here. Some literature has noted that it may reduce the possibility of side-effects present in long-term antibiotic usage while having similar efficiency on rosacea symptom reduction [74].
The one negative some users have reported is the strong odor, which can persist even after the solution has been thoroughly washed off.
In addition to standalone sulfur usage, combination with sodium sulfacetamide (which also has anti-inflammatory and antibacterial properties [75]) appears to further enhance effectiveness and reduce the amount of sulfur required to achieve similar results [76]. However, some may still prefer sulfur on its own to limit the possibility of adverse effects.
Azelaic Acid
Azelaic acid is another popular acne treatment that has been shown to be effective in rosacea treatment, with some studies suggesting it can even be a viable alternative to topical metronidazole [77].
The main benefits highlighted with this treatment option is its natural origin and reduced potential for long-term side effects [78].
Another interesting factor of azeliac acid is that it’s naturally produced by Malassezia furfur (a yeast though to play a central role in seborrheic dermatitis) [79], but topical application has been shown to improve seborrheic dermatitis symptoms [80].
Potential Natural Treatment Approaches
User reports suggest that many of the common treatments can produce inconsistent results and some fear the potential for unwanted side-effects. Because of this, a search for alternative natural treatment approaches has continued.
Strictly based on the available literature, two natural approaches stand out from the rest:
- Niacinamide and Zinc Supplementation
Individuals given a daily supplement containing 750mg nicotinamide, 25mg zinc, 1.5mg copper and 500 micrograms folic acid showed improvements comparable to oral antibiotic therapy [81]. Effectiveness is believed to be related to the supplements anti-inflammatory properties, bacteriostatic effects, and ability to reduce sebum production [82]. - Licorice Extract
Known for it’s anti-inflammatory potential, licorice has been used throughout history for a variety of health concerns. Topical ointments containing certain extracts of the plant have been shown to produce significant reductions in redness and inflammation in mild cases of rosacea [83], atopic dermatitis [84] and redness caused by UV damage [85].
In addition to these, other approaches have also been speculated to be of use based on their beneficial properties on skin healing and inflammation reduction [86, 87, 88]. These include:
- Green tea washes and extracts
- Topical aloe vera solutions
- Topical chamomile formulations
- Turmeric supplementation
- Mushroom extracts
- Probiotics
- Omega 3s
But even though anecdotal reports of effectiveness do exist, a lack of examination for their specific usage in rosacea remains.
Section Summary
This section provided an in-depth overview of rosacea and how it compares to seborrheic dermatitis. Though unanswered questions remain, the content discussed can serve as a good starting point for any one effected by the condition.
Key takeaways of this section include:
- Rosacea is a skin condition that causes excessive inflammation of the facial skin (commonly restricted to specific areas) and is believed to have a strong genetic component
- Though the condition often accompanies seborrheic dermatitis, the two conditions have many fundamental differences; biggest difference is related to the role of sebum
- Rosacea has been categorized into four individual variants and pin-pointing the exact one your facing, can play a big role in determining which treatment choice is most applicable
- Blood flow irregularities, altered immune system functioning, UV damage, structural changes/abnormalities of the skin, demodex mites, digestive issues and dietary factors have been implicated as potential causes
- Long term usage of steroids can trigger symptoms that mimic rosacea; in these cases, restricting steroid usage usually results in gradual symptom improvement
- Though there has been a tremendous amount of studies trying to pin-point a single cause, no consensus has been reached and variation amongst individuals may be responsible
- Most common treatment options include: avoidance of triggering elements (foods, beverages, stress, certain medication), topical and systemic antibiotics, and immune system modulating agents
- Natural approaches have received much less attention, but options such as sulfur, azelaic acid, supplementation with niacinamide and zinc, and topical ointments containing licorice extracts may be worth considering
{kind=link}
No Comments
Be the first to start a conversation